What is Airway Obstruction (in Children)?
Airway Obstruction in children is characterised by mouth breathing, snoring, tooth grinding, bedwetting, allergies or frequent ear or other ear/nose/throat infections. Breathing is primary and when obstruction is present, the body adapts muscle positions to create as much airway space as possible. If muscle positions are not normal, then bones grow abnormally.
**This blog post has been posted with permission from Dr. Derek Mahony.
List of symptoms associated with Airway Obstruction in Children
Facial asymmetries and some TMJ dysfunctions (jaw joint problems) can also be attributed to orofacial muscle imbalances and deviate tongue postures due to airway interferences. The following is list of symptoms associated with airway obstruction in children:
- Open mouth position (with possible open-bite)
- Narrow nares
- Short upper lip
- Prominent upper incisors (front Teeth)
- V-shaped maxilla (upper jaw), high palatal vault.
- Pouting lower lip
- Class II occlusal relationship (lower teeth in front of upper teeth)(adenoid problem)
- Class III occlusal relationship (Lower teeth in front of upper teeth)(tonsil problem)
- Chronic chapped and cracked lips
- Tongue held in low mouth position
- Creases on nose (allergic salute)
- Aggravated allergies
- Gummy Smile and red swollen gum tissues
- Allergic Shiners (constant dark circles under the eyes)
- Excessive Snoring at night
Orofacial Growth
85% of orofacial growth is accomplished by the age of twelve. Therefore, early identification of airway interferences, with diagnosis of the underlying cause, is essential to prevent orofacial growth abnormalities. If you, your dentist, dental hygienist or paediatrician observe any of the above symptoms and suspect possible airway obstruction in your child, evaluation by an ENT (ear, nose and throat) physician should be undertaken.
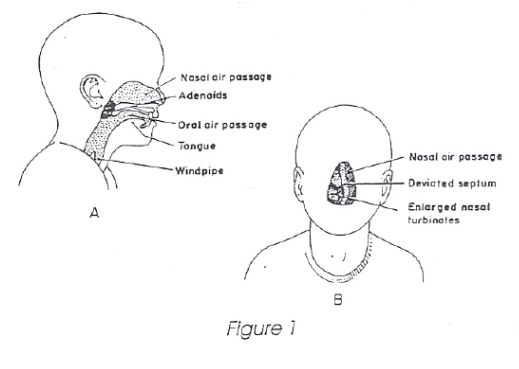
Did you know that the way your child breathes can affect the development of his or her jaws and facial structure influencing how the teeth fit together? Normal breathing should occur through the nose with the mouth closed. However, if the nasal passage is somehow obstructed, mouth breathing often results. Generally, nasal airway obstruction is caused by one or more of the following: (see figure 1)
- Enlarged adenoids
- Nasal blockage due to swollen tissue, allergies or polyps
- Underdeveloped nasal passages and/or underdeveloped jaw and cheekbones
- Deviated nasal septum
- Enlarged nasal turbinates
All of the above causes the child to breath with his or her mouth open. This open mouth posture causes the facial muscles to generate unnatural constrictive forces on the underlying bony structures (See Figure 2A). Narrowing and elongation of the upper jaw often is the result of such forces (see Figure 2B). In addition, the jaws tend to grow
apart, often causing front open bites which affect the position of the tongue and other facial structures. 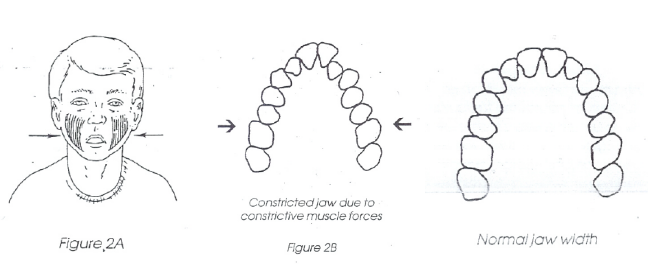
Also, because the lower jaw is dropped for mouth breathing, it tends not only to grow apart from the upper jaw, but also becomes positioned further back than normal, causing an overbite (Figure 2C).

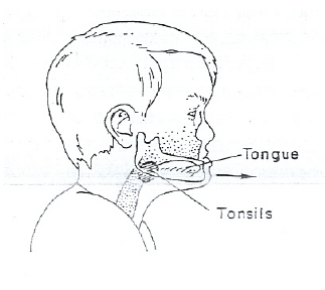
How the tongue rets in the mouth can also negatively affect facial growth. The tongue at rest should be high in the mouth which stimulates normal growth of the maxilla (upper jaw). Enlarged tonsils force the tongue in a downward and forward position which pushes on the lower jaw and the lower teeth (tongue trust). This in turn can contribute to prognathism (protruding of the lower jaw) by overstimulating jaw growth (Figure 3).
Please keep in mind that there are many other factors beside airway considerations that affect dental-facial development (ie. genetics, muscular tone, tooth and jaw sizes, allergies etc). There for addressing just these airway interferences will not always guarantee correction of dento-facial problems. However, if airway interferences are eliminated before facial growth is completed, a suitable environment will be establishes to promote a more normal development of the orofacial structures. This can eliminate or simplify the need for extensive orthodontic treatment. Also in cases where airway interferences have been eliminated, relapse of orthodontic treatment is greatly reduced. The results include not only a more stable dentition and bite, but also a more pleasing facial appearance for your child.
The following professional references have been provided for you and your medical practitioner if they would like to know more about the effects of airway obstruction upon facial growth.
- McNamara, J.A. and Ribbens, K.A. eds., 1979. Naso-respiratory function and craniofacial growth (Vol. 9). Center for Human Growth and Development, University of Michigan.
- Linder-Aronson, S., Woodside, D.G. and Lundströ, A., 1986. Mandibular growth direction following adenoidectomy. American journal of orthodontics, 89(4), pp.273-284.
- Shapiro, P.A., 1988. Effects of nasal obstruction on facial development. Journal of Allergy and Clinical Immunology, 81(5), pp.967-971.
- Meredith, G.M., 1988. Airway and dentofacial development. American Journal of Rhinology, 2(1), pp.33-41.
- Richter, H.J., 1987. Obstruction of the pediatric upper airway. Ear, nose, & throat journal, 66(5), p.209.
- Petit, H., 1987. Upper airway problems and pre-orthodontic orthopedics. Ear, nose, & throat journal, 66(6), p.228.
- Gray, L.P., 1987. Rapid maxillary expansion and impaired nasal respiration. Ear, nose, & throat journal, 66(6), p.248.
- Timms, D.J., 1990. Rapid maxillary expansion in the treatment of nocturnal enuresis. The Angle Orthodontist, 60(3), pp.229-233.
- Timms, D.J., 1987. Rapid maxillary expansion in the treatment of nasal obstruction and respiratory disease. Ear, nose, & throat journal, 66(6), p.242.